For years, PRP has been caught between promise and inconsistency
Strong biological rationale, contradictory clinical results. The paradox is now resolved. Four converging lines of published evidence show that PRP failures were preparation failures: insufficient dose, discarded proteins, centrifugation damage, and uncontrolled variability.
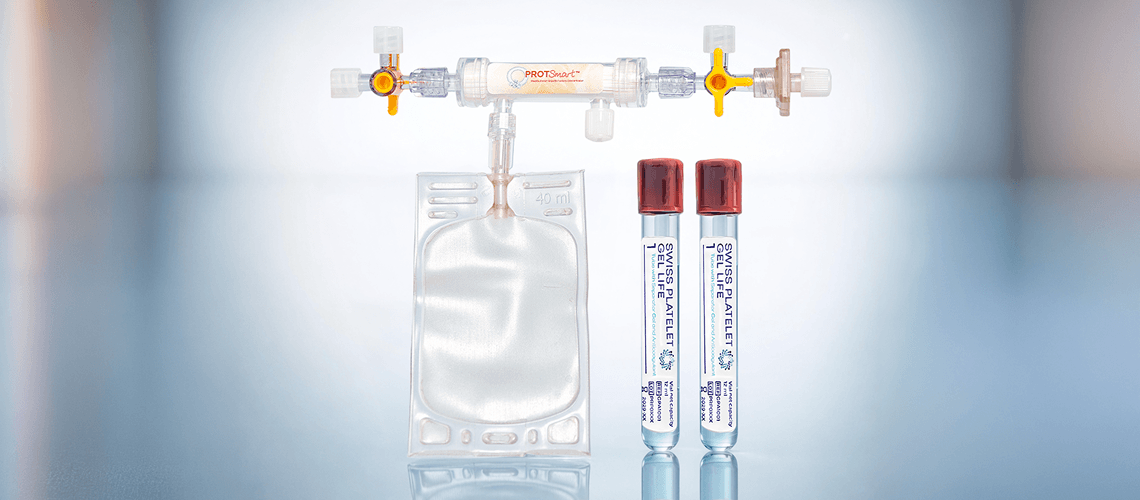
PCX is the first PRP system designed for what the science now demands — therapeutic platelet dose AND concentrated plasma proteins, from a single 24 mL blood draw, with no second centrifugation spin and no plasma discarded.
Concentrate by retaining. Not by discarding.
Four Convergences —
Between 2024 and 2026, four independent lines of published evidence converged to reveal that conventional PRP preparation — whether single-spin or doublespin — has fundamental limitations that no amount of incremental improvement can overcome.
Published evidence now proves that platelet dose — not concentration ratio — determines whether PRP works or fails.
A 2025 meta-analysis of 18 placebo-controlled RCTs (1,995 patients) found that highplatelet PRP maintained clinically significant benefit through 12 months, while low-platelet PRP never exceeded the minimum clinically important difference for pain at any timepoint (Bensa, Filardo et al., Am J Sports Med, 2025). In lateral epicondylitis, 58.5% of all between-study heterogeneity was explained by platelet concentration alone — low-dose PRP showed zero benefit; high dose PRP showed strong benefit (Oeding et al., Am J Sports Med, 2025).
A multi-society Delphi consensus achieved 90–99% expert agreement: PRP below 2,500 x 10⁶ platelets is not effective, while PRP above 5,000 x 10⁶ shows positive clinical effect at both 6 and 12 months (Hubbard et al., Arthroscopy, 2024).
WHAT THIS MEANS:
Single-spin gel tubes — producing 0.5–1.7 billion platelets per preparation — are now demonstrably sub-therapeutic by published standards. A 2024 study found standard gel tube preparation achieved only 1.06x concentration, with approximately 65% of platelets trapped below the gel barrier (Batra et al., J Cosmet Dermatol, 2024).
The field has recognized that platelets alone are insufficient. Plasma proteins constitute a second, independent therapeutic axis — and every conventional PRP system ignores it.
A 2026 paper from researchers in regenerative medicine stated it directly: “The platelet is not the drug; it is the delivery system. This limited view, which equates platelet number with regenerative efficacy, has become deeply ingrained in both clinical practice and industry marketing” (Costa et al., Life, 2026).
Published research identifies critical therapeutic proteins that reside in plasma, not in platelets: IGF-1 (the only growth factor independently correlated with cell proliferation — and it does not correlate with platelet levels); HGF (anti-fibrotic signaling); alpha-2-macroglobulin (the master protease inhibitor); and fibrinogen (which creates the 3D scaffold that binds and slowly releases 15+ growth factors) (Beitia et al. 2023; Everts et al. 2024).
WHAT THIS MEANS:
Single-spin systems contain these proteins but at concentrations too dilute to be therapeutically meaningful. Double-spin systems discard 60–80% of plasma as “platelet-poor plasma” — permanently losing IGF-1, HGF, A2M, fibrinogen, fibronectin, and extracellular vesicles.
Published research demonstrates that high-speed centrifugation — the method every double-spin system relies on — damages the very cells it aims to concentrate.
P-selectin expression (the standard marker of premature platelet activation) rises from 11–15% at low centrifugation speeds to 43–56% at the speeds used in double-spin protocols (Söderström et al., Clin Chem Lab Med, 2016). When platelets activate during processing, they release their growth factors into the surrounding plasma — which is then discarded. A study comparing concentration methods found platelet activation of 5.2% with filtration versus 12.2% with centrifugation (Burns et al., PLoS One, 2018; P = .005).
Published research on ultrafiltration concluded explicitly: “None of these [centrifugation] methods have the ability to concentrate extraplatelet molecules” (Mercader Ruiz et al., J Clin Med, 2023). Ultrafiltration is not a better centrifuge — it is a fundamentally different separation paradigm.
WHAT THIS MEANS:
No centrifugation-based system — single-spin or double-spin — can concentrate plasma proteins. Only ultrafiltration can.
An updated 2025 systematic review found that fewer than 20% of Level I/II orthopedic PRP studies provided a reproducible preparation protocol, and only 26.6% reported final product composition (Lim et al., Arthroscopy, 2025). The DEPA classification documented a 25-fold variation in platelet dose (0.21–5.43 billion) across 20 preparations from the same starting material (Magalon et al., BMJ Open Sport Exerc Med, 2016). A 2020 review of 36 commercial systems found “large heterogeneity” and “absence of biological quality control” (Magalon et al., Platelets, 2020).
The root cause: operator-dependent manual processing. Judging plasma layers, pipetting buffy coat, resuspending pellets — these techniques create variability that centrifugation cannot eliminate because it is the centrifugation method that introduces the variability.
WHAT THIS MEANS:
When membrane pore size determines what stays and what passes, operator skill becomes irrelevant to product composition. Physics-governed separation is the only path to reproducible PRP.
A Fundamentally
PCX separates plasma isolation from concentration — using the right technology for each.
Where single-spin systems stop at insufficient concentration and double-spin systems trade platelet quality for quantity, PCX assigns each task to the technology suited for it.
STEP 1: GEL SEPARATION —
Isolate Plasma

A single centrifugation step separates red and white blood cells below a proprietary gel barrier. Platelet-rich plasma — with its full protein complement intact — remains above the gel. This step isolates plasma. It does not attempt to concentrate it. No high-speed spin. No platelet pelleting.
Unlike single-spin-only systems, PCX does not stop here. The plasma above the gel — which in a standalone gel tube would be the final product at just 1–2x concentration — becomes the starting material for Step 2.
STEP 2: PROSMART 2 ULTRAFILTRATION —
Concentrate Everything

The isolated plasma is concentrated through the ProtSmart 2 device — a hollow fiber membrane with a 15 kDa molecular weight cutoff (~5 nm pore size), manufactured by Medica S.p.A. (Italy) using MediSulfone® polysulfone. Water and small electrolytes pass through into a waste bag. Platelets, growth factors, plasma proteins, and extracellular vesicles are retained and concentrated — together, in a single unified process.
Unlike double-spin systems, no additional centrifugation is needed. There is no platelet pelleting, no high-speed spin, no PPP generation, and no plasma discard.
THE THREE-WAY COMPARISON

Why the
ProtSmart 2 membrane: ~5 nm pores. Platelets: 2,000–4,000 nm.
The ProtSmart 2 membrane has an effective pore size of approximately 5 nm. A platelet is 2,000–4,000 nm in diameter — 400 to 800 times larger than the pore. It physically cannot pass through. This is not a performance claim. It is filtration physics.
The same principle applies to every therapeutic component above the 15 kDa molecular weight cutoff — plasma proteins, growth factors, and extracellular vesicles are all retained. Only water (18 Da), electrolytes (23–39 Da), and metabolic waste (glucose, urea, creatinine) pass through. None of the removed components contribute to PRP’s therapeutic effect.
RETAINED AND CONCENTRATED:

Platelets (2,000–4,000 nm) — Alpha-2-macroglobulin (720 kDa) — Fibronectin (440 kDa) — Fibrinogen (340 kDa) — IgG (150 kDa) — HGF (90 kDa) — Albumin (66.5 kDa) — VEGF (38 45 kDa) — PDGF (24–29 kDa) — TGF-β (25 kDa) — Extracellular vesicles (30–1,000 nm) — IGF-1 (>98% bound to carrier proteins in 25–150 kDa complexes → retained)
MEMBRANE SAFETY:

The ProtSmart 2 uses MediSulfone® polysulfone — the most widely used membrane material for blood contact applications worldwide, with decades of safety data from hemodialysis. Published research confirms that hollow fiber filtration does not activate platelets more than centrifugation (Arnaud et al. 2003), and hydrophilically modified polysulfone reduces platelet adhesion by over 99% (Yamaka et al. 2017).
Beyond Platelets
All conventional PRP systems — single-spin and double-spin — focus exclusively on platelet concentration. Published research now shows this is insufficient. PCX is the only PRP system designed to concentrate the full plasma protein profile alongside platelets in a single process.
What PCX concentrates that conventional systems miss:

Alpha-2-macroglobulin (A2M)
The master protease inhibitor that neutralizes cartilage degrading enzymes. A 2025 study showed ultrafiltration concentrated A2M 4.3x while maintaining biological activity.
IGF-1
The only growth factor independently correlated with cell proliferation in PRP studies. Does not come from platelets — resides in plasma. Concentrated by ultrafiltration but lost by every double-spin system and too dilute in single-spin products (Beitia et al. 2023; Mercader Ruiz et al. 2023).
Fibrinogen
Polymerizes into a fibrin scaffold that binds 15+ growth factors for sustained release. Creates the 3D matrix essential for cell homing and tissue architecture.
HGF
Anti-fibrotic signaling and epithelial cell motility. Resides in plasma, not platelets.
Extracellular vesicles
Intercellular signaling particles carrying miRNAs, proteins, and growth factors. 70–80% of circulating EVs are platelet-derived but partition into the PPP fraction that double-spin systems discard.Published support:
Research using the same ProtSmart ultrafiltration membrane achieved protein concentrations of 12–16 g/dL (~2x normal) and 52% wound surface area reduction in severe pressure ulcers (Mazzucco et al., Front Bioeng Biotechnol, 2024). Ultrafiltrationenriched PRP showed significantly enhanced cell proliferation versus standard PRP (Mercader Ruiz et al., J Clin Med, 2023; P < 0.01). Independent research confirms that enriching PRP with plasma proteins enhances biological activity with significant antiinflammatory effects (Sánchez et al., Nat Sci Rep, 2025).
PCX by SWISS concept —
The concentration power of ultrafiltration. The simplicity of a single-spin workflow.
Specifications:
~15 MIN — Processing time 5.5–6x — Projected concentration* ≥89% — Projected recovery* 24 ML — Blood volume ~2x — Projected protein enrichment*
*Design-based projections from gel separation physics and membrane retention characteristics. Validation studies in development.
PCX requires only a standard laboratory centrifuge — no specialized PRP equipment, no capital investment beyond the disposable kit. The kit includes 2x Swiss Platelet Gel Life tubes (12 mL each, medical-grade glass with separator gel, anticoagulant, and calibrated vacuum) and 1x ProtSmart 2 ultrafiltration device (15 kDa hollow fiber membrane, MediSulfone® polysulfone by Medica S.p.A., Italy).
How PCX compares to gel tubes alone:
Swiss Platelet Gel Life tubes without ProtSmart 2 produce standard single-spin PRP — approximately 2–5x baseline concentration. The ProtSmart 2 transforms the output: concentrating the recovered plasma by ~3.4x through water removal, achieving the projected 5.5–6x total concentration with ~2x protein enrichment that single-spin systems cannot match and double-spin systems sacrifice plasma proteins to achieve.
System
Comparison table:

*PCX values are design-based projections. Validation studies in development.
The pattern is clear: single-spin systems offer simplicity but sub-therapeutic dose. Double-spin systems achieve higher concentrations but damage platelets and discard proteins. PCX is designed to achieve the concentration of double-spin systems with the simplicity of single-spin — while adding the protein enrichment that neither approach delivers.
1 Mandle RJ. BSR comparison study, 2016. Non-peer-reviewed laboratory report; n=4. 2 Degen RM et al. HSS J. 2017;13(1):75–80. 3 Magalon J et al. Arthroscopy. 2014;30(5):629–638. 4 Jildeh TR et al. Cureus. 2022;14(8):e28498. 2 of 4 ART samples fell below baseline. 5 Inyang OE et al. JAAD. 2021;85(3):788–790. Peer-reviewed, n=40.
The Science Behind
Clinical
PCX by SWISS concept is designed for use across multiple clinical disciplines. The system’s concentrated 3–4 mL output from just 24 mL of blood is ideally matched to indications requiring precise, small-volume delivery of high-concentration, protein enriched PRP.
The following reflects published PRP field research, not PCX-specific outcomes. PCXspecific validation studies are in development.
Evidence: Strong — 119+ RCTs, ~76,000 patients
PRP outperforms hyaluronic acid: 44.7% WOMAC improvement versus 12.6% across 18 Level 1 RCTs (Belk et al. 2021). High-platelet PRP maintains benefit through 12 months; low platelet PRP fades after 6 months (Bensa et al. 2025). ESSKA-ORBIT 2024: Grade A — “a valid treatment option and possible first-line injectable.”
Volume required: 2–3 mL intra-articular
PCX fit: Excellent — full treatment from one kit
Protocol: 3 injections at 2–4 week intervals; annual maintenance
Protein enrichment relevance: HIGH — A2M (protease inhibition), IGF-1 (cartilage cell survival), fibrinogen (intra-articular scaffold)
Evidence: Strong — Lateral epicondylitis, plantar fasciitis
PRP significantly outperforms corticosteroids at ≥6 months for lateral epicondylitis (VAS MD: −2.18, P < 0.0001) and plantar fasciitis (P < 0.00001). 58.5% of outcome variability in LE explained by platelet concentration alone (Oeding et al. 2025). LP-PRP preferred.
Volume required: 1–2 mL peritendinous/intratendinous
PCX fit: Excellent — can treat multiple sites from one kit
Protocol: 1–3 injections at 2–4 week intervals
Protein enrichment relevance: HIGH — IGF-1 (tendon cell proliferation), fibrinogen (scaffold for tendon repair)
Evidence: Strong— CMC, ankle, wrist, AC joint
Small joint capsules cannot tolerate large-volume injections. PCX’s concentrated low volume output is specifically suited to these anatomies.
Volume required: 0.5–1.5 mL per joint
PCX fit: Excellent — multiple joints from one kit
Protocol: 1–3 injections at 2–4 week intervals
Protein enrichment relevance: HIGH — same mechanisms as knee OA in a smaller space
Evidence: Moderate-Strong — 13 meta-analyses
PRP augmentation lowers retear rates (RR 0.38, P = 0.0009) and improves short-term function (Ahmad et al. 2022). Recommended for single-row repair.
Volume required: 3–5 mL as gel or fibrin matrix at repair site
PCX fit: Good — 3–4 mL covers most single-row applications. Activated into gel with CaCl₂.
Protocol: Single application at time of arthroscopic repair
Evidence: Moderate — 5 studies meta-analysis
PRP augmentation reduced meniscal repair failure from 25.7% to 9.9% (OR 0.31, P < 0.0005).
Volume required: 2–4 mL as gel at repair site
PCX fit: Good — full output as activated gel
Protocol: Single application during arthroscopic repair
Evidence: Moderate — 6 RCTs
PRP reduced hamstring return-to-play by 8.6 days (P = 0.045; Nakagawa et al. 2026).
Volume required: 3–6 mL image-guided
PCX fit: Good for moderate injuries (3–4 mL). Large muscle tears may benefit from higher volume.
Protocol: Single injection within 48 hours of injury; image-guided
Evidence: Moderate short-term, weak long-term — Pain reduction at 3–6 months but no benefit at 12 months. Volume: 4–10 mL — may require two kits for intra-articular + tunnel protocols. Note: this is one indication where PCX’s 3–4 mL may be limiting for comprehensive augmentation.
Evidence: Emerging-Moderate — VAS improved at 24 months (11 studies).
Volume: 2–4 mL — good fit.
Evidence: Moderate-High — 43 RCTs, 1,877 participants
+25–28 hairs/cm. versus placebo. 65–87% response rates. Patient satisfaction >90%. Dose-response confirmed: 42% density increase at >1M plt/μL versus 16% at lower concentrations (Singh 2023). PRP comparable to minoxidil with significantly higher patient satisfaction (OR: 2.77).
Volume required: 3–5 mL via mesotherapy (0.05–0.1 mL/cm.)
PCX fit: Excellent — 3–4 mL covers a typical treatment area
Protocol: 3 monthly sessions; maintenance every 3–6 months; LP-PRP preferred
Protein enrichment relevance: VERY HIGH — IGF-1 is the only growth factor correlated with proliferation and does NOT come from platelets. Balding follicles produce less IGF-1. Only ultrafiltration concentrates it.
Evidence: Moderate — MN+PRP: 3x higher odds of >50% improvement
A 2024 network meta-analysis (24 RCTs, 1,546 patients) ranked laser + PRP best (SUCRA: 98.4%). Microneedling + PRP yields 3x higher odds of >50% improvement versus microneedling alone.
Volume required: 2–3 mL topical application post-microneedling
PCX fit: Excellent — volume matches treatment area for face
Protocol: 3–4 sessions at 4-week intervals
Protein enrichment relevance: HIGH — fibrinogen creates scaffold in microchannels for sustained growth factor release; EVs carry collagen-regulating miRNAs
Evidence: Mixed — Histological improvements consistent; clinical RCT evidence mixed
Histological studies consistently show increased collagen deposition. However, the Alam et al. 2024 Mayo Clinic RCT found no significant improvement in skin laxity versus saline. Best evidence supports combination protocols (MN+PRP, laser+PRP).
Volume required: 2–4 mL (mesotherapy + topical)
PCX fit: Good — full output for comprehensive facial treatment
Honest positioning: Lead with combination protocols. Standalone rejuvenation remains an evolving indication.
Evidence: Moderate — 10 studies, 395 patients
mMASI score reduction of 1.18 points (P = 0.02). PRP via microneedling most effective (Zhao et al. 2021).
Volume required: 2–3 mL via microneedling
PCX fit: Excellent
Protocol: 3–4 sessions at 4-week intervals
Protein enrichment relevance: HIGH — TGF-β modulation of melanocyte activity
Evidence: Moderate — 48 studies, 2,186 patients
Average repigmentation of 58.7%, especially effective combined with CO₂ laser or excimer laser (Jafarzadeh et al. 2024).
Volume required: 0.1 mL per injection point, intradermal
PCX fit: Excellent — 3–4 mL covers extensive treatment areas at 0.1 mL/point
Protocol: Multiple sessions combined with phototherapy
Protein enrichment relevance: HIGH — melanocyte growth factors
Evidence: Emerging — 8 studies
PRP improved POSAS scores for keloids (P < 0.05) with fewer side effects than triamcinolone. CTGF reduction of 40–50%.
Volume required: 1–3 mL intralesional
PCX fit: Good — treat multiple scars from one kit
Protocol: 3–4 sessions at monthly intervals
Evidence: Early — 6 studies, “poor” evidence quality.
Volume: 3–4 mL via microneedling — good fit.
Evidence: Emerging — 13 studies; ~67% improved at 1 year
A 2025 systematic review showed PRP improves symptoms and quality of life. Placebocontrolled RCT using ~4 mL PRP currently underway.
Volume required: 3–4 mL subdermal
PCX fit: Good — volume matches the ongoing RCT protocol
Protocol: 3 sessions at monthly intervals
Evidence: Strong — 29 RCTs, 2,198 wounds
Complete wound closure OR 5.32. DFU-specific: RR 1.42, healing time reduced by 3.13 weeks, amputation rate reduced by 65% (Deng et al. 2023). Protein-enriched PRP using the same ProtSmart membrane: 52% wound area reduction at 6 weeks in severe pressure ulcers (Mazzucco et al. 2024).
Volume required: 2–4 mL topical gel per application
PCX fit: Excellent — activated PRP gel applied directly to wound bed
Protocol: Application every 1–2 weeks until healing; CaCl₂ activation for gel formation
Protein enrichment relevance: VERY HIGH — concentrated fibrinogen creates the scaffold, fibronectin enables cell adhesion, A2M prevents wound degradation. This is where protein enrichment has the most direct published clinical support (Mazzucco 2024).
Evidence: Moderate — 9 RCTs
PRP reduced healing time by 6.68 days and wound infection by 82% (2025 meta-analysis).
Volume required: 2–5 mL depending on burn area
PCX fit: Good for localized burns; extensive burns may need multiple kits
Protocol: Topical application as activated gel at dressing changes.
Evidence: Strong to Moderate — Umbrella review of 40 systematic reviews (Acerra et al. 2025)
Extraction socket healing: significantly reduced pain, swelling, and dry socket (33 RCTs, 2,277 sockets). Periodontal regeneration: CAL gain +0.76 mm, PD reduction +0.53 mm (12 RCTs). TMJ disorders: significant pain reduction (SMD −0.99, P < 0.00001; 6 RCTs). Implant osseointegration: improved early stability
Volume required: 1–3 mL per surgical site
PCX fit: Excellent — concentrated output ideal for small surgical fields
Protocol: Single application at time of surgery (extraction, implant, periodontal)
Protein enrichment relevance: HIGH — fibrinogen scaffold for bone formation, growth factors for osseointegration
Peyronie’s Disease
Evidence: Early — 1 interim RCT, 1 prospective cohort. Curvature reduced from 40° to 25° (P = 0.047).
Volume: 0.5 mL intralesional — excellent PCX fit.
Evidence: Moderate-Strong — 8 RCTs, 678 patients
Intrauterine PRP infusion increases endometrial thickness by 1.23 mm, clinical pregnancy rate RR 2.04, and live birth rate RR 2.46 (Liu et al. 2024). Cycle cancellation reduced by 54%.
Volume required: 0.5–1 mL intrauterine infusion
PCX fit: Excellent — small volume, high concentration ideal for intrauterine use
Protocol: 1–2 infusions in the cycle preceding embryo transfer
Protein enrichment relevance: HIGH — growth factors promote endometrial angiogenesis and receptivity
Evidence: Controversial — Positive observational but negative RCTs (Barrenetxea 2024, Herlihy 2024).
Volume: 1–2 mL intraovarian — excellent fit, but indication currently unsupported by rigorous evidence.
PRP Eye Drops
Evidence: Moderate — 16 RCTs in network meta-analysis
PRP drops significantly outperform artificial tears for corneal fluorescein staining and rank highest for corneal damage improvement (Zhang et al. 2024). Effective for dry eye disease, corneal epithelial defects, and persistent corneal ulcers. PRP contains significantly higher EGF, PDGF, NGF, and fibronectin than autologous serum.
Volume required: 3–4 mL PRP → diluted to 20–50% concentration → provides 2–4 weeks of eye drops
PCX fit: Excellent — one processing yields weeks of therapy
Protocol: 5–6 drops/day; continuous use for chronic conditions
Protein enrichment relevance: VERY HIGH — EGF, NGF, and fibronectin are the active epitheliotrophic factors. Concentrated PRP produces a more potent eye drop preparation.
Evidence: Moderate — 3 RCTs
PRP significantly outperforms corticosteroids at 6 months for lumbar disc herniation (pain MD −1.51, P < 0.00001; Ermawan et al. 2025). Steroids peak early and decline; PRP builds over time — the same pattern seen in tendinopathies.
Volume required: 3 mL transforaminal epidural
PCX fit: Excellent — direct match for onekit, one-treatment
Protocol: Single injection; repeat at 6–12 months if needed
Protein enrichment relevance: HIGH — anti-inflammatory proteins (A2M, albumin) for nerve root protection
Evidence: Moderate — Level II RCT + prospective studies
71% success rate with LP-PRP (Zhang et al. 2023). Sustained pain and function improvement at 1 year (Tuakli-Wosornu 2016, Level I RCT). Higher PRP concentration (>10x) produces significantly better outcomes than lower concentration (P = 0.004, Centeno et al. 2022).
Volume required: 1–2 mL per disc
PCX fit: Excellent — can treat 2 disc levels from one kit
Protocol: Single injection per level; image-guided
Protein enrichment relevance: VERY HIGH — concentration matters here (>10x significantly better). PCX’s 5.5–6x is well positioned. A2M for disc protease inhibition.
Evidence: Moderate-Strong — 9+ RCTs, 400+ patients
PRP surpasses corticosteroids beyond 6 months for both severity and function (P = 0.04 severity, P < 0.00001 function; 2025 indirect meta-analysis). Significant SSS and FSS improvements at 1, 3, and 6 months (Du et al. 2025, 7 RCTs).
Volume required: 1–2 mL ultrasound-guided perineural
PCX fit: Excellent — treat bilateral CTS from one kit
Protocol: Single injection; repeat at 6–12 months
Protein enrichment relevance: VERY HIGH — NGF, PDGF, VEGF, IGF-1 are directly neurotrophic. Optimal concentration for Schwann cell proliferation is 4.5x (Zheng et al. 2020) — close to PCX’s projected 5.5–6x.
Evidence: Moderate — 3 RCTs
Significant improvements in pain, numbness, and nerve conduction velocity at 1, 3, and 6 months (Hassanien et al. 2020; P ≤ 0.001). PRP superior to pregabalin for pain and sleep (Anwar 2024).
Volume required: 2–3 mL perineural
PCX fit: Excellent
Protocol: Single injection; repeat at 3–6 months
Veterinary Applications
Evidence: Moderate for equine and canine — PRP is “likely efficacious” for equine OA (Peng et al. 2024).
Canine OA: significant pain improvement with 1–2 mL (Alves et al. 2021).
PCX fit: excellent for small animal joints (1–2 mL); limited for large equine joints (stifle: ~8 mL).
Beyond Concentration
Concentration ratio alone is misleading. A system achieving 6x with only 40% recovery delivers fewer total platelets than PCX’s projected 5.5x at ≥89% recovery.
And concentration tells you nothing about what else is in the product. A 7x double-spin PRP has concentrated platelets but zero concentrated proteins — the second therapeutic axis is missing. A 1.5x single-spin PRP contains everything but concentrates nothing adequately.
PCX is designed to deliver high recovery, efficient concentration, AND protein enrichment — all three, from 24 mL of blood.
Total Platelets Delivered Beyond Concentration

Total Platelet Recovery by Method
Evidence
PCX’s performance specifications — ≥89% platelet recovery, 5.5–6x concentration, ~2x protein enrichment — are design-based projections derived from gel separation physics and the validated retention characteristics of the 15 kDa ProtSmart 2 ultrafiltration membrane.
The ultrafiltration approach is supported by published peer-reviewed research:
- Same ProtSmart membrane: 52% wound area reduction in severe pressure ulcers (Mazzucco et al. 2024)
- UF concentrates IGF-1 and HGF with enhanced cell proliferation (Mercader Ruiz et al. 2023)
- IGF-1 is the only growth factor correlated with proliferation; does not come from platelets (Beitia et al. 2023)
- Protein-rich PRP matrices described as “multi-purpose biological platforms” (Everts et al. 2024)
The innovation context is supported by converging published evidence:
- Dose determines outcome (Berrigan 2025; Oeding 2025; Bensa 2025)
- “The platelet is not the drug; it is the delivery system” (Costa et al. 2026)
- Filtration activates platelets less than centrifugation (Burns et al. 2018)
- <20% of PRP studies provide reproducible protocols (Lim et al. 2025)
PCX-specific validation studies are in development.
References
1. Berrigan WA et al. Platelet dose and knee OA outcomes. Arthroscopy. 2025;41(3):809–817.
2. Bensa AF, Filardo G et al. PRP vs placebo for knee OA. Am J Sports Med. 2025;53(3):745–754.
3. Oeding JF et al. Platelet concentration explains variability in lateral epicondylitis. Am J Sports Med. 2025.
4. Patel S et al. Conventional vs superdose PRP. Orthop J Sports Med. 2024;12(2).
5. Corsini AC et al. Re-evaluating PRP dosing. J Clin Med. 2025;14(8):2714.
6. Hubbard MJ et al. Delphi consensus on PRP. Arthroscopy. 2024;40(2):470–477.
7. Costa M et al. Beyond platelet count. Life. 2026;16(2):188.
8. Rothrauff BB et al. PRP in MSK disease 2025 and beyond. Am J Sports Med. 2026.
9. Mazzucco L et al. Protein-enriched filtered PRP. Front Bioeng Biotechnol. 2024;11:1279149.
10. Mercader Ruiz J et al. UF for plasma growth factors. J Clin Med. 2023;12:5941.
11. Beitia M et al. PRP bioactivity: more than platelets. Int J Mol Sci. 2023;24:5367.
12. Everts PA et al. Protein-rich PRP matrices. Int J Mol Sci. 2024;25:7914.
13. Sánchez M et al. Plasma molecule concentration improves PRP. Nat Sci Rep. 2025;15:4523.
14. Söderström AC et al. Centrifugation and platelet activation. Clin Chem Lab Med. 2016;54(12):1913–1920.
15. Burns KA et al. Filtration vs centrifugation. PLoS One. 2018;13(1):e0190827.
16. Arnaud FG et al. Hollow fiber filtration. Platelets. 2003;14(3):131–137.
17. Yamaka T et al. Polysulfone hemocompatibility. Contrib Nephrol. 2017;189:222–229.
18. Lim SY et al. PRP protocols: an updated review. Arthroscopy. 2025;41:821–834.
19. Chahla J et al. Call for PRP standardization. JBJS. 2017;99(20):1769–1779.
20. Magalon J et al. DEPA classification. BMJ Open Sport Exerc Med. 2016;2(1):e000060.
21. Magalon J et al. Technical review of PRP devices. Platelets. 2020;32(2):200–208.
22. Belk JW et al. PRP vs HA for knee OA. Am J Sports Med. 2021;49(1):249–260.
23. Laver L et al. ESSKA-ORBIT consensus. KSSTA. 2024;32(4):783–797.
24. Bensa AF et al. Safety of injectables. KSSTA. 2025. (76,061 patients.)
25. Marx RE. J Oral Maxillofac Surg. 2004;62(4):489–496.
26. Batra R et al. Where have all the platelets gone? J Cosmet Dermatol. 2024.
27. Deng C et al. PRP for diabetic foot ulcers. J Orthop Surg Res. 2023;18(1):370.
28. Anitua E et al. PRP for AGA: 43 RCTs. Dermatol Ther. 2025.
29. Castillo TN et al. Am J Sports Med. 2011;39(2):266–271.
30. Magalon J et al. Arthroscopy. 2014;30(5):629–638.
31. Degen RM et al. HSS J. 2017;13(1):75–80.
32. Jildeh TR et al. Cureus. 2022;14(8):e28498.
33. Inyang OE et al. JAAD. 2021;85(3):788–790.
34. Singh S, Singh B. Dose-response in PRP for AGA. IJDVL. 2023.